Inside the Novice Nurse Brain: Bridging the Experience Gap
2026-07-27 01:00:16By Rose O. Sherman, EdD, RN, NEA-BC, FAAN
For nurse leaders and preceptors, watching newly licensed nurses struggle can feel baffling. You see a patient in bed 4 showing subtle signs of early sepsis, and your brain instantly triggers an action plan. Meanwhile, your novice nurse is hyper-focused on completing a routine medication pass on time, completely missing the trend in decompensating vital signs. What looks like a lack of focus or slow critical thinking isn’t a motivation problem—it’s a neurological and cognitive processing reality. With many units now dominated by novice staff, nurse leaders are grappling with how to best accelerate their learning to improve patient safety.
Understanding how the novice nurse brain processes information allows leaders to build targeted scaffolding that speeds up clinical competency development while reducing turnover. Dr. Patricia Benner’s Novice to Expert framework provides guidance on how to think about this. New nurses rely entirely on step-by-step rules because they lack contextual clinical experience.
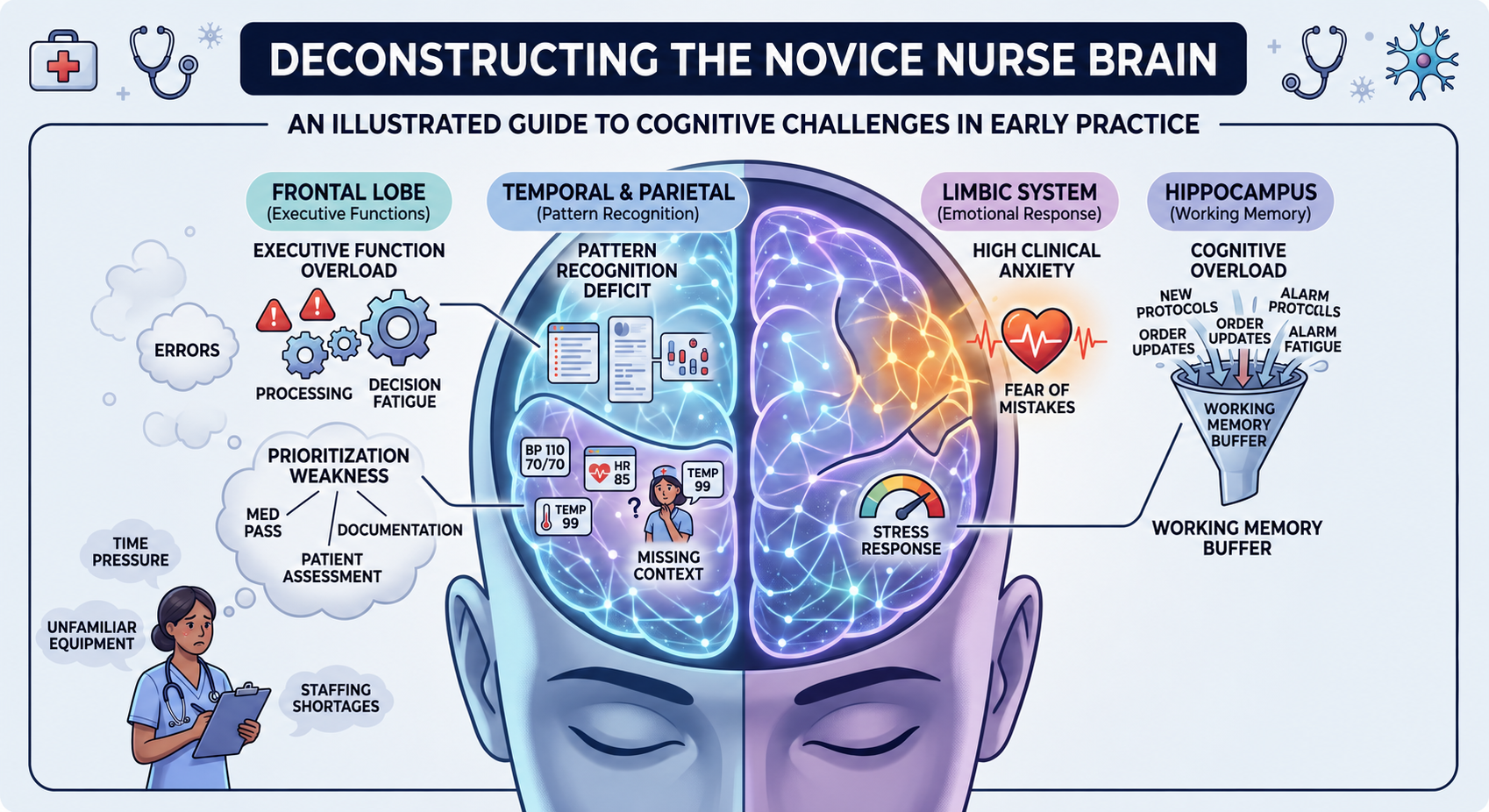
Below are five cognitive hurdles new nurses face every shift and strategies leaders can use to mitigate them:
- Cognitive Overload – For most of us, our working memory can only hold 4 to 7 items at a time. An expert nurse bundles tasks (e.g., assessing lung sounds while checking IV lines and asking about pain). A novice nurse processes every single item as a standalone, high-energy mental task. This leads them to appear disorganized, document slowly, feel constantly “behind,” and miss obvious physical cues. To help with cognitive overload, nurse leaders and preceptors should help reduce unnecessary mental bandwidth by using standardized bedside shift report templates, pre-printed task checklists, and unit-specific “cheat sheets.” Reducing choices about what to do next helps cognitive overload.
- Pattern Recognition Deficits – Expert nurses rely on illness scripts—mental models built over years of seeing hundreds of patients. Novices have textbook knowledge, but they cannot yet connect isolated symptoms (a slight drop in blood pressure, mild confusion, low urine output) into a unified picture of clinical decline. To help build pattern recognition, leaders and preceptors need to shift their questions. Instead of asking “What are their vitals?”, ask “Which vital sign concerns you most right now, and why?” Practice explicit “thinking aloud” during complex patient cases. Ask “What is your biggest concern about this patient right now, and what evidence is driving that?”
- Decision Fatigue – An experienced nurse makes hundreds of clinical choices on autopilot. A novice nurse must consciously debate every micro-decision: Should I flush the line before or after? Do I call the doctor now or wait 10 minutes? Which patient do I see first? By hour 6 of a 12-hour shift, their executive functioning drops sharply. This is exhausting to the brain and leads to paralysis by analysis, frequent interruptions to ask basic questions, or simple mistakes late in the shift. To combat this, leaders need to establish explicit decision algorithms and red flag alerts. Provide clear “If/Then” guidelines for common unit situations (e.g., If SBP drops below 90, do X, then notify Y) to protect executive function for true emergencies.
- Prioritization Weakness – To a novice nurse brain without clinical context, an impending stat lab draw, a demanding family member, a routine dressing change, and a patient asking for water all carry equal weight. You then see novices focusing on easy, checklist-style tasks (like charting) while critical clinical needs get delayed. Nurse leaders and preceptors should implement the “2-Minute Mid-Shift Huddle.” and do a quick 120-second priority check at 11:00 and 15:00: “Tell me your top 2 priorities for the next two hours.” Ask questions such as “If two of your patients need you at the exact same moment right now, how will you decide who gets seen first?”
- Clinical Anxiety – High-stakes environments trigger the amygdala (the brain’s threat center). When adrenaline surges, the prefrontal cortex—where critical thinking occurs—functions less effectively. This is why we see novices demonstrate hyper-defensiveness when receiving feedback, or physical symptoms of stress during shift handoffs. Nurse leaders and preceptors must normalize the learning curve. Psychological safety is required for learning. Reframe mistakes made in good faith into learning opportunities through structured, non-punitive debriefs. Ask questions like “What was a moment today where you felt completely out of your depth—and what did you do to navigate it?” or “What is one clinical decision you made today that you feel really proud of?”
I sometimes become frustrated when I hear nurse leaders talk about the need to make novices more work ready before entering practice. The gaps discussed above take time to bridge and extensive clinical exposure. This does not happen overnight. The real change today is that in acute care, we have a novice dense workforce on so many units. Their brains are different than experienced staff and we need to acknowledge that.
© emergingrnleader.com 2026
To effectively lead through these challenges and others, nurse leaders need new tools and strategies. Let me help you as I have helped hundreds of organizations over the past five years. Please contact me at roseosherman@outlook.com to book a workshop or keynote for your team. Not seeing what you want on this list? Feel free to reach out, and I am happy to design a custom program to meet your needs.
Brand New For 2026 and Already Receiving Rave Reviews – Staying Power Building a Culture of Retention in the New World of Work
Brand New for 2026 and Already Popular – The Inverted Pyramid: Leading Teams of Novice Nurses The Inverted Pyramid WS Information Sheet
Our Most Popular Right Now –The New World of Work Workshop
A Leader Favorite – Building Bridges Not Walls: Leading Multigenerational Work Teams – Click Here for More Information Building Bridges Not Walls
A Must-Read Book in 2026 – Click Here to Buy

Developing Red Flag Lists in Acute Care
2026-07-20 01:00:22By Rose O. Sherman, EdD, RN, NEA-BC, FAAN
One of the challenges of having a novice-dense workforce in acute care is teaching them to recognize clinical deterioration and, more crucially, to overcome the “intimidated silence” that often occurs in these environments. As I do the Inverted Pyramid Workshops across the country, so many nurse managers have talked with me about this issue. Without experienced staff to coach novices in clinical surveillance, small changes in a patient’s condition that indicate more serious underlying issues are not being identified. Transfers to higher levels of care increase, as does length of stay.
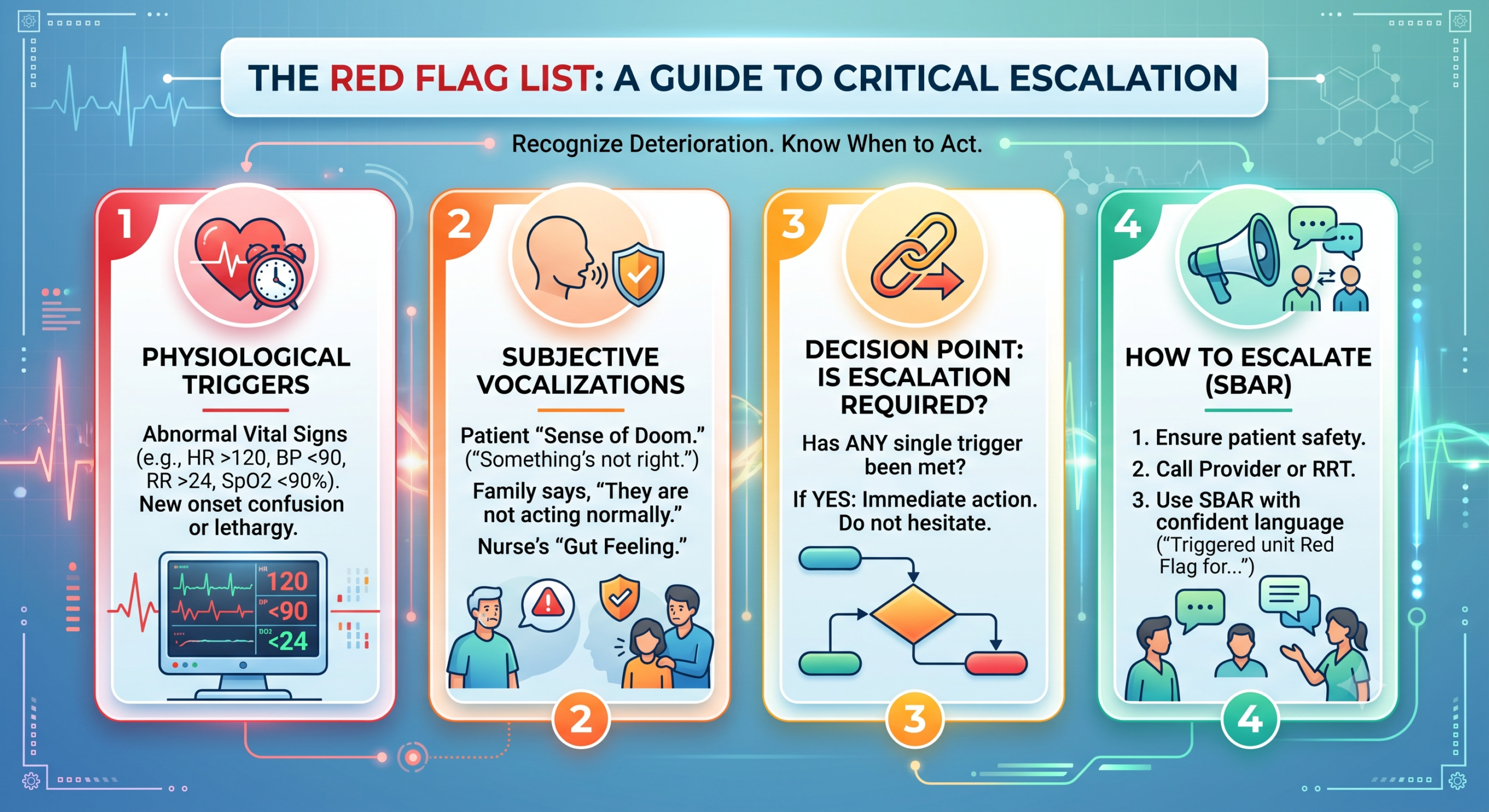
Because novice nurses frequently struggle to differentiate between a patient who is “expectedly sick” and one who is actively decompensating, a Red Flag List provides objective, permission-giving criteria to escalate care. Red Flag lists provide decision scaffolding for novice staff. A Red Flag List is a clear, single-page document that explicitly outlines the clinical triggers, patient status changes, or operational events that must be escalated to the Nurse in Charge, the Patient’s Physician, or the Rapid Response Team.
By removing the ambiguity around when to call for help, you eliminate the novice’s fear of “bothering” the charge nurse or the physician while creating an ironclad safety net for clinical risk management. An orthopedic nurse manager recently explained how she developed this Red Flag List to improve care on her unit.
I began to notice that my novices were not anticipating some of the critical complications that we see in orthopedics, such as compartment syndrome, vascular compromise, or thromboembolic events. They were falling into the trap of thinking – of course their leg hurts terribly, they just had total knee arthroplasty. After meeting with stakeholders, I determined that novice nurses on my unit faced a specific challenge: distinguishing expected post-operative pain from limb- or life-threatening emergencies. Their ability to connect these dots on their own just was not there. We needed more of a safety net so we designed a Red Flag List.
The orthopedic-specific Red Flag List they designed is designed draws a hard line in the sand, helping them differentiate expected surgical recovery from critical complications like compartment syndrome, neurovascular compromise, and thromboembolic events. It is a yellow/red flag list that requires nurses to notify the Charge Nurse, Rapid Response Team, and/or the Physician immediately if a patient exhibits any of the following:
| Assessment Category | Yellow Flag – Notify Charge Nurse | Red Flag – Notify Provider – Call RRT |
| Vascular Status – Operated Extremity | Capillary refill: 3–4 seconds. Extremity feels slightly cooler than the unoperated side. Patient reports mild, intermittent “pins and needles” | Capillary refill: greater than 4 seconds. Extremity is cold, pale, cyanotic, or mottled. New, progressive, or continuous numbness/paresthesia. Inability to move digits (e.g., new foot drop or loss of finger extension). Absence of peripheral pulse (even by Doppler) |
| Pain Trajectory | Pain is 8–10/10 but decreases slightly with ordered opioids. Patient requires maximum allowed PRN breakthrough doses | Severe, deep, throbbing pain that is completely unresponsive to maximum opioid doses. Pain that increases rapidly and is disproportionate to the surgical procedure. Pain elicited by passive stretching of the muscles (e.g., gently moving the toes/fingers) |
| Surgical Site & Drains | The incision dressing is saturated with serosanguineous fluid and requires reinforcement. Hemovac or Jackson-Pratt (JP) drain output: 100–150 mL over 2 hours | Active, bright red (frank) blood rapidly saturating the dressing Hemovac/JP drain output: greater than 200 mL in a single hour. A rapidly expanding, tense, hard hematoma or visible bulging around the surgical site |
| Thromboembolic & Pulmonary (DVT, PE, & Fat Embolism)
|
Unilateral calf tenderness or localized swelling in the non-operated leg. Heart Rate: 100–115 bpm | Sudden onset of SOB, tachypnea (RR > 24), or chest pain. SpO2 less than 92% on room air (or a sudden 4% drop from baseline), Petechial rash across the chest, neck, or axilla (classic sign of Fat Embolism Syndrome), Heart rate greater than 120 bpm |
This manager was wise enough to anticipate that defining when to call is only half the battle; the menu must also define how to communicate the risk efficiently. She required the use of SBAR directly on the handout so the novice knows exactly what information to have ready when they escalate. Novices, she observed, often worry about waking up a surgeon at 02:00. You have to give them this exact script to structure their call:
S (Situation): “Dr. Brooks, this is Susan on the Orthopedic Unit. I am calling to escalate care for Mr. Miller in Room 304, status post total knee arthroplasty today. He has actively triggered our unit Red Flag List for suspected Compartment Syndrome.”
B (Background): “He returned from the PACU at 16:00. His neurovascular checks were baseline normal until the last 30 minutes.”
A (Assessment): “He is experiencing severe, localized calf pain rated at a 10/10 that did not respond to the IV Dilaudid given 45 minutes ago. His calf is visibly tense and hard to the touch. Most importantly, he screams with pain upon passive dorsiflexion of his toes. His pedal pulse is still palpable, but weak.”
R (Recommendation): “Because he meets the explicit Red Flag criteria for compartment syndrome, I need an immediate bedside evaluation for a compartment pressure check and potential emergency fasciotomy. I have already verified he is NPO. Can you be here within 15 minutes, or should I contact the on-call hospitalist?
She realized that part of the challenge in using Red Flag lists is that you also need to educate the surgeons. When a novice calls a physician using the Red Flag Menu, his/her response dictates whether they will utilize it next time or hide their concern out of fear. This manager asked physicians to avoid saying, “Why are you calling me?” If the escalation is unnecessary, I told them to contact me and I will coach the nurse through the decision they made. These lists are not foolproof she noted – her unit went through many iterations but they are a good start to improving patient safety and novice nurse confidence.
© emergingrnleader.com 2026
To effectively lead through these challenges and others, nurse leaders need new tools and strategies. Let me help you as I have helped hundreds of organizations over the past five years. Please contact me at roseosherman@outlook.com to book a workshop or keynote for your team. Not seeing what you want on this list? Feel free to reach out, and I am happy to design a custom program to meet your needs.
Brand New For 2026 and Already Receiving Rave Reviews – Staying Power Building a Culture of Retention in the New World of Work
Brand New for 2026 and Already Popular – The Inverted Pyramid: Leading Teams of Novice Nurses The Inverted Pyramid WS Information Sheet
Our Most Popular Right Now –The New World of Work Workshop
A Leader Favorite – Building Bridges Not Walls: Leading Multigenerational Work Teams – Click Here for More Information Building Bridges Not Walls
A Must-Read Book in 2026 – Click Here to Buy
Adopting a Nurse Leader Coach Mindset
2026-07-16 01:00:57By Rose O. Sherman, EdD, RN, NEA-BC, FAAN
When nurse leaders ask me today what they need to do to futureproof their leadership, I recommend that they adopt a leader-coach mindset. You may believe as a leader that you already do this, but don’t be so sure. If you walk through almost any clinical unit, you will hear a variation of the same scene: A frustrated young nurse approaches their manager with a problem. The manager, eager to be helpful (and desperate to keep the shift moving), immediately says, “Here is what you need to do…” It is an understandable instinct. As nurse leaders, we are conditioned to solve problems quickly. We view swift fixing as a sign of strong, supportive leadership.
The problem with doing this is that we are failing to develop the critical thinking skills of our staff. Inevitably, they will be back asking the same question again because they have not learned to think through problems on their own. This is exhausting for the leader and does not empower our staff. If we want to build highly resilient, autonomous, and critical-thinking nursing teams, we have to change our approach. We need to transition from the “Fixer” mentality to a “Nurse Leader Coach Mindset”.
Interestingly, today’s nursing workforce wants its leaders to use less of a traditional style and more of a coaching approach. Generation Z is far less likely to take advice from their leaders or parents than from peers or social influencers. Yet, the transition from a traditional leader to a team coach is not always smooth. It means you need to be a lot less Superman and a lot more Yoda.
What is a Coaching Mindset?
A coaching mindset is not about having all the answers; it is about having the right questions. It is a deliberate shift from directing to developing. When you adopt a coaching mindset, your goal is no longer just solving the immediate issue in front of you. Instead, you are using the daily challenges of the unit as real-time opportunities to grow your nurses’ critical thinking, clinical judgment, and professional confidence.
Making this shift successfully relies on the following four essential behaviors:
-
Presence: Entering every conversation with full attention, non-judgment, and genuine empathy.
-
Deep Listening: Giving your staff the actual space to fully express their thoughts before jumping in.
-
Mindset: Staying curious to inspire growth and self-reflection, rather than just collecting factual data.
-
Powerful Questions: Using open-ended prompts that encourage reflection and independent problem-solving.
Busy nurse leaders often tell me, “I don’t have time to sit down for formal coaching sessions – I can’t fit this into my day.” The good news is that coaching does not require a scheduled, meeting in your office. The most impactful coaching happens during short micro-interventions while rounding, in the hallway or at the nurses’ station. To do this effectively, consider the following strategies:
© emergingrnleader.com 2026
To effectively lead through these challenges and others, nurse leaders need new tools and strategies. Let me help you as I have helped hundreds of organizations over the past five years. Please contact me at roseosherman@outlook.com to book a workshop or keynote for your team. Not seeing what you want on this list? Feel free to reach out, and I am happy to design a custom program to meet your needs.
Brand New For 2026 and Already Receiving Rave Reviews – Staying Power Building a Culture of Retention in the New World of Work
Brand New for 2026 and Already Popular – The Inverted Pyramid: Leading Teams of Novice Nurses The Inverted Pyramid WS Information Sheet
Our Most Popular Right Now –The New World of Work Workshop
A Leader Favorite – Building Bridges Not Walls: Leading Multigenerational Work Teams – Click Here for More Information Building Bridges Not Walls
A Must-Read Book in 2026 – Click Here to Buy
Invitation for Nurse Executive Leaders: Confidential Research Interview related to Preparing Healthcare for the Future
2026-07-14 01:00:26Please consider participating in this important research study. Link for Eligibility Criteria

Navigating the Dunning-Krueger Effect on Units with an Inverse Pyramid of Experience
2026-07-13 01:00:42By Rose O. Sherman, EdD, RN, NEA-BC, FAAN
A nurse leader recently asked me how to manage overconfidence with her novice team. She told me that many of her newest nurses had challenges taking feedback. She further explained: “Ironically, some of my new graduates think they are very high performers when they are not. I think they are comparing themselves to other nurses with a similar level of experience on the unit. They don’t seem to know or sometimes care what they don’t know, and this is frustrating our preceptors. How do I manage this on a very novice-dense unit?”
The Dunning-Kruger Effect Defined
The Dunning-Kruger Effect is a cognitive bias in which people who are new to or unskilled at something drastically overestimate their abilities, while true experts often underestimate theirs. Simply put: The less you know about a subject, the less qualified you are to judge how little you know. The challenge for the nurse leader who asked the question is that she now has a unit dominated by novices. If not managed, this cognitive bias among nursing staff could become a major patient safety risk.
The Dunning-Krueger Effect is not new in nursing, but historically, it was not a major issue because we had many experienced nurses in acute care who could rein in overconfident new graduates by pointing out what they had overlooked. On many units today, that built-in safety net no longer exists, and much of this coaching falls to nurse leaders and preceptors.
Coaching Overconfident Staff
Coaching an overconfident new graduate requires leadership finesse. If you push too hard, you risk crushing their spirit and triggering defensive behavior. Other the other hand, if you are too hands-off, patient safety is compromised. The first important concept as you think about coaching nurses who seem overconfident as an outcome of the Dunning-Krueger Effect is to understand that you are not witnessing arrogance. What you are seeing is a biological cognitive limit. Because they lack clinical pattern recognition, they literally cannot see what they don’t know. These nurses are at risk of missing subtle patient decompensations because they assume everything is under control. They don’t call for help because they don’t realize help is needed.
Some Good Leader Interventions to Counter the Dunning-Krueger Effect
- Don’t ask an overconfident novice – “Do you have any questions?” (to which a confident novice will always say no).
- Shift toward active cognitive rounding. Ask the nurse to articulate their clinical reasoning by using active, inquiry-based dialogue. Instead of saying “Let me know if you need help with this admission.” Instead say, “This patient has a complex history. Tell me the three worst-case scenarios you’re monitoring for during this shift, and what your first action will be if they happen.”
- Create objective, non-negotiable clinical triggers that mandate a second set of eyes, bypassing a novice’s subjective confidence. Overconfident individuals often perceive subjective feedback as a personal critique or “micromanagement.” To bypass their defensive ego, anchor your coaching in objective data, policies, and evidence-based checklists. Example – “Our policy requires a dual-sign-off for high-alert meds. It doesn’t matter how comfortable you feel with it; it’s a safety guardrail for all of us.”
- Coach preceptors to look for the “overconfident new grad” Teach preceptors about the Dunning-Krueger Effect so they can gently but firmly guide the nurse to reality before a clinical error occurs. When an experienced preceptor performs a task, 80% of their critical thinking happens invisibly in their head. The overconfident new grad only sees the physical action and thinks, “Oh, that looks easy.” Coach preceptors to narrate their own internal monologues to expose the hidden layers of clinical practice. Example “I am giving this medication, but notice how I’m checking the patient’s trending potassium levels first, even though the morning lab was normal? I’m doing that because their urine output dropped last hour. See how those two things connect?” By making the invisible visible, you demonstrate to the new nurse just how much nuance they are currently overlooking.
- Praise the Ask. New graduates often view asking for help as a confession of weakness or failure. They overcompensate by acting like they have everything under control. Leaders must actively flip this script. It is important as a leader to normalize the Dunning-Krueger Effect and work with new graduates to avoid this cognitive bias (as you would any other cognitive bias). When a new graduate actually does ask a question or requests a second pair of eyes, reward that behavior immediately and publicly. Say – “I love that you called the charge nurse to double-check that rhythm. Recognizing when a situation requires a team approach is exactly what highly competent, safe nurses do. Great catch.”
The Inverse Pyramid of Experience is the reality of the modern healthcare workforce. But an inexperienced staff only becomes a dangerous staff when leadership fails to manage the gaps in confidence and competence.
© emergingrnleader.com 2026
To effectively lead through these challenges and others, nurse leaders need new tools and strategies. Let me help you as I have helped hundreds of organizations over the past five years. Please contact me at roseosherman@outlook.com to book a workshop or keynote for your team. Not seeing what you want on this list? Feel free to reach out, and I am happy to design a custom program to meet your needs.
Brand New For 2026 and Already Receiving Rave Reviews – Staying Power Building a Culture of Retention in the New World of Work
Brand New for 2026 and Already Popular – The Inverted Pyramid: Leading Teams of Novice Nurses The Inverted Pyramid WS Information Sheet
Our Most Popular Right Now –The New World of Work Workshop
A Leader Favorite – Building Bridges Not Walls: Leading Multigenerational Work Teams – Click Here for More Information Building Bridges Not Walls
A Must-Read Book in 2026 – Click Here to Buy

[news count=”4″ pagination=”2″ terms=”24,22″][/news]


 LinkedIn
LinkedIn